




What is a Diabetic Foot Ulcer?
A diabetic foot ulcer is an open sore or wound that occurs in approximately 15 percent of patients with diabetes and is commonly located on the bottom of the foot. Of those who develop a foot ulcer, 6 percent will be hospitalized due to infection or other ulcer-related complication.
Diabetes is the leading cause of non-traumatic lower extremity amputation, and approximately 14-24 percent of patients with diabetes who develop a foot ulcer will require an amputation. Foot ulceration is the cause of the absolute majority of diabetes-related amputations. Research has shown, however, that the development of a foot ulcer is preventable and when they occur rapid treatment helps prognosis- here is were podiatry plays an important role.
Causes
Anyone who has diabetes can develop a foot ulcer with ethnicity and race also playing a role. People who use insulin are at higher risk of developing a foot ulcer, as are patients with diabetes-related kidney, eye, and heart disease. Being overweight and using alcohol and tobacco also plays a role in the development of foot ulcers.
Ulcers form due to a combination of factors, such as lack of feeling in the foot (neuropathy), poor circulation, foot deformities, irritation (such as friction or pressure), and trauma, as well as duration of diabetes (especially uncontrolled diabetes). Patients who have diabetes for many years can develop neuropathy, a reduced or complete lack of ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time. The nerve damage often can occur without pain, and one may not even be aware of the problem. Your podiatrist can test your feet for neuropathy with a simple, painless tool called a monofilament.
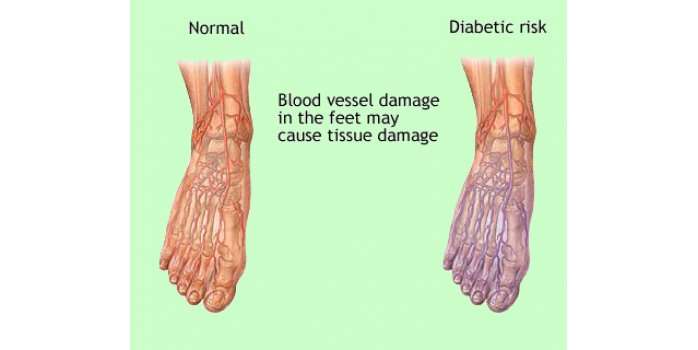
Vascular disease can complicate a foot ulcer, reducing the body’s ability to heal and increasing the risk for an infection. Elevations in blood glucose can reduce the body’s ability to fight off a potential infection and also slow healing. Your podiatrist can test your peripheral circulation utilizing painless methods, including Doppler ultrasound and ABPI.
Symptoms
Because many people who develop foot ulcers have lost the ability to feel pain, pain is not a common symptom. Many times, the first thing you may notice is some drainage on your socks. Redness and swelling may also be associated with the ulceration and, if it has progressed significantly, odor may be present, indicating infection.
When to Visit a Podiatrist
Once an ulcer is noticed, seek podiatric medical care immediately. Foot ulcers in patients with diabetes should be immediately treated to reduce the risk of infection and amputation, improve function and quality of life, and reduce health-care costs.
Podiatry care is important because patients will benefit from:
- Diagnosis on the type of ulcer (e.g. neuropathic, venous ulcer) and diagnose the underlying cause (e.g. peripheral arterial disease).
- Debridement (remove dead skin) around and/or on the ulcer as this is known to aid in the healing process.
- Off- loading of the ulcerative area and other areas of excessive pressure depending on the patients’ biomechanics and the results from a foot pressure scan.
- Footwear advice depending on the patient and any foot deformities present.
Diagnosis and Treatment
The primary goal in the treatment of foot ulcers is to obtain healing as soon as possible. The faster the healing, the less chance for an infection.
There are several key factors in the appropriate treatment of a diabetic foot ulcer:
- Prevention of infection
- Taking the pressure off the area, called “off-loading”
- Removing dead skin and tissue, called “debridement”
- Applying medication or dressings to the ulcer
- Managing blood glucose and other health problems
Not all ulcers are infected; however, your podiatrist may consult or refer you to your G.P if an infection is present for an antibiotics prescription. To keep an ulcer from becoming infected, it is important to:
- keep blood glucose levels under tight control;
- keep the ulcer clean and bandaged;
- cleanse the wound daily, using a wound dressing or bandage; and
- avoid walking barefoot.
For optimum healing, ulcers, especially those on the bottom of the foot, must be “off-loaded.” You may be asked to wear special footgear, or a brace, specialized castings, or orthotics/ insoles. These devices will reduce the pressure and irritation to the area with the ulcer and help to speed the healing process.
The science of wound care has advanced significantly over the past ten years. The old thought of “let the air get at it” is now known to be harmful to healing. We know that wounds and ulcers heal faster, with a lower risk of infection, if they are kept covered and moist. The use of full-strength betadine, hydrogen peroxide, whirlpools, and soaking are not recommended, as these practices could lead to further complications.
Appropriate wound management includes the use of dressings and topically-applied medications. Products range from normal saline to growth factors, ulcer dressings, and skin substitutes that have been shown to be highly effective in healing foot ulcers.
For a wound to heal, there must be adequate circulation to the ulcerated area. Your podiatrist can determine circulation levels with noninvasive tests.
Tightly controlling blood glucose is of the utmost importance during the treatment of a diabetic foot ulcer. Working closely with a medical doctor or endocrinologist to control blood glucose will enhance healing and reduce the risk of complications.
Healing time depends on a variety of factors, such as wound size and location, pressure on the wound from walking or standing, swelling, circulation, blood glucose levels, wound care, and what is being applied to the wound. Healing may occur within weeks or require several months.
Surgical Options: A majority of non-infected foot ulcers are treated without surgery; however, if this treatment method fails, surgical management may be appropriate. Examples of surgical care to remove pressure on the affected area include shaving or excision of bone(s) and the correction of various deformities, such as hammertoes, bunions, or bony “bumps.” Revascularization surgery may be considered when a diabetic ulcer cannot heal and occurs secondary to limb ischemia due to peripheral vascular disease.
Prevention
The best way to treat a diabetic foot ulcer is to prevent its development in the first place. Recommended guidelines include seeing a podiatrist on a regular basis. Your podiatrist can determine if you are at high risk for developing a foot ulcer and implement strategies for prevention.
You are at high risk if you have or do the following:
- Neuropathy
- Poor circulation
- A foot deformity (e.g., bunion, hammer toe)
- Wear inappropriate shoes
- Uncontrolled blood sugar
- History of a previous foot ulceration
Reducing additional risk factors, such as smoking, drinking alcohol, high cholesterol, and elevated blood glucose, are important in prevention and treatment of a diabetic foot ulcer. Wearing the appropriate shoes and socks will go a long way in reducing risks. Your podiatrist can provide guidance in selecting the proper shoes.
Learning how to check your feet is crucial so that you can find a potential problem as early as possible. Inspect your feet every day—especially the sole and between the toes—for cuts, bruises, cracks, blisters, redness, ulcers, and any sign of abnormality. Each time you visit a podiatrist or your health care provider, remove your shoes and socks so your feet can be examined. Any problems that are discovered should be referred or reported to your podiatrist as soon as possible; no matter how simple they may seem to you.
Further reading for health care professionals:
Systematic Review of Wound Management
http://europepmc.org/abstract/MED/11074391/reload=0;jsessionid=Js8VgC1YOSFm5QI6j0tn.24
The Association between Callus Formation, high pressures and neuropathy in diabetic foot ulceration
Diagnosis and Treatment of Diabetic Foot Infections: